


Cornea and ocular surface / Keratoprosthesis
Keratoprosthesis, what is it?
Keratoprosthesis involves replacing a diseased cornea with an artificial cornea, produced using excellent quality, fully transparent materials with properties and a tolerance that is perfectly suited to the patient.
This procedure is performed on patients who reject natural corneas from donors or who suffer from cornea problems or bilateral corneal surface disorders, such as conjunctivalisation secondary to total limbal deficiency or severe dry eye.
Types of keratoprosthesis
There are different prosthesis designs and surgical techniques available, which are designed to improve anatomical and functional results.
Osteo-odonto keratoprosthesis
Osteo-odonto keratoprosthesis (OOKP) is an ophthalmological surgical technique that allows us to recover vision in a blind eye from a piece of tooth, and it is performed when a cornea transplant has failed, or when it is not a viable option.
Ideal candidates for this surgery are patients who are suffering corneal blindness as a result of auto-immune disease or chemical burns, for example, but it is not suitable for patients who are blind from birth or who suffer from glaucoma or some form of retinal disease.
First stage
[Read more]
Second stage
[Read more]
Third stage
[Read more]
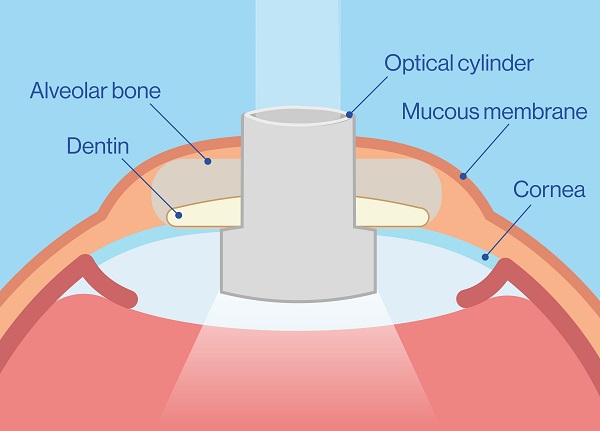
For this autologous transplant we use a lamina from the root of the upper canine tooth as a biological support for an optical cylinder. An ultrasound scan needs to be performed beforehand, as well as effective management of intraocular pressure.
The surgical procedure is carried out in three stages, with the first two being performed during the same session. The third stage is carried out after a 2-3 month integration period, to ensure that the new prosthesis is viable for the eye.
Expectations and results
In good anatomical conditions, 75% of patients will keep the prosthesis for up to 20 years. Patients may reach up to 100% vision if their optic nerve and retina are in perfect condition. This means that the visual prognosis depends not only on the condition of the cornea, but also that of the retina and optic nerve.
The risks involved in the surgery are the potential loss of the teeth next to the canine tooth and bleeding in the operated areas.
After the surgery, there may be a risk of infection, glaucoma, membranes, extrusions or retinal problems.
It is a procedure that was created in the 1960s by an Italian ophthalmology surgeon called Benedetto Strampelli, and was then perfected by Professor Giancarlo Falcinelli. Although its success rate is quite high, it is not widely used currently, as not many ophthalmologists around the world perform it; in Spain, Dr. María Fideliz de la Paz is the only surgeon specialised in performing it and is renowned worldwide for his expertise.
Tibial bone osteo-keratoprosthesis
→ The tibial bone osteo-keratoprosthesis (tibial KPRO) is a surgical technique that also uses bone tissue to support the eye.
→ The tibial bone extracted from the leg measures around 10 mm in diameter. As with the keratoprosthesis using a canine tooth, the optical cylinder is implanted in the middle of the bone.
→ This assembled piece is implanted in a space below the lower eyelid to be covered in fibrovascular tissue for 3 months.
In good anatomical conditions, over 50% of patients will keep the prosthesis for up to 10 years. As with the keratoprosthesis performed with a tooth, the visual result is always dependent on the condition of the retina and the optic nerve.
The potential complications of this procedure are the same as with the tooth. There may be bleeding during or after the surgery, particularly in patients with coagulation disorders. One difference is that there is a slightly higher chance of extrusion than in the procedure involving a tooth, as the bone is reabsorbed slightly faster than the tooth.
Boston keratoprosthesis
Boston keratoprosthesis (Boston Kpro) is a procedure often chosen by patients that need a corneal transplant but suffer from significant limbal deficiency, or have rejected corneal transplants in the past, so would have a lower chance of success with a traditional keratoplasty.
It will also be necessary to ensure that these patients have an adequate eye surface, good eyelid function and suitable tear production, and that their optic nerve and retina are in good condition.
This treatment is used on patients with the following eye disorders, among others:
→ Failed cornea grafts.
→ Burns to the eyes (from chemicals or heat).
→ Bullous keratopathy.
→ Herpetic leukaemia.
→ Certain cases of uveitis.
→ Insufficient limbal due to incorrect use of contact lenses.
→ Aniridia.
This type of keratoprosthesis involves the following:
→ A titanium plate with several holes.
→ An optical cylinder (made of high grade PMMA plastic) that acts as a lens.
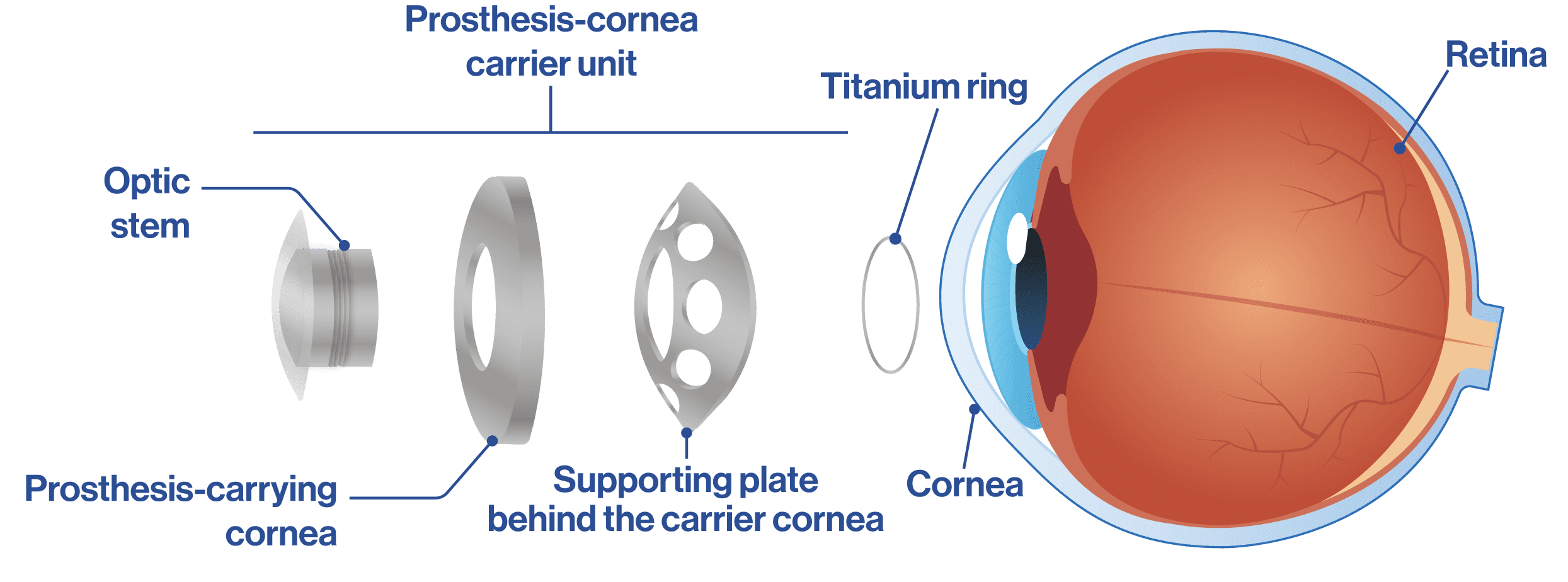
· Both pieces are mounted on a donor cornea that, once fitted together, is fitted onto a titanium ring so that the entire structure is securely fastened and the cornea does not come loose.
· The prosthesis is then implanted in the eye with stitches, as with a cornea transplant.
· The visual prognosis for these patients is better as the retina and optic nerve are in good condition. Glaucoma, infection, membranes and inflammation may be present in these cases.
· Effective post-operative care is essential for the patient’s entire life, to ensure healthy development.
Ophthalmologists who specialise in keratoprosthesis
Our ophthalmologists who specialise in these techniques have been recognised by the Harvard Massachusetts Eye and Ear Infirmary as “Distinguished Boston KPro Surgeons”.


